
Anatomy
ANATOMY
 In the axilla, the median nerve lies superficially on the biceps side of the axillary artery. It crosses the artery in the lower arm to lie medial to the brachial artery in the antecubital fossa. In the forearm, the nerve passes deep to the superficial flexors, giving rise to the anterior interosseous nerve and more distally, a superficial palmar branch. It then enters the hand via the carpal tunnel.
In the axilla, the median nerve lies superficially on the biceps side of the axillary artery. It crosses the artery in the lower arm to lie medial to the brachial artery in the antecubital fossa. In the forearm, the nerve passes deep to the superficial flexors, giving rise to the anterior interosseous nerve and more distally, a superficial palmar branch. It then enters the hand via the carpal tunnel.
Positioning
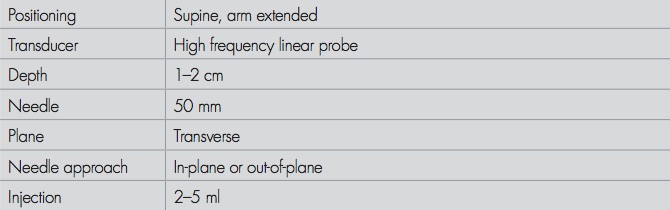
POSITIONING
Position the patient supine with arm abducted and elbow extended. Place the transducer transversely across the antecubital fossa at the level of the elbow crease. Identify the brachial artery (pulsatile anechoic), the median nerve lies medial to the artery as a distinct hyperechoic structure (ovoid or almond shaped), at a varying distance 0.5–2 cm, slightly deeper lying on the pronator teres muscle.
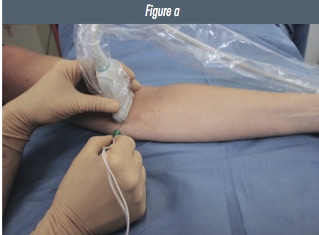
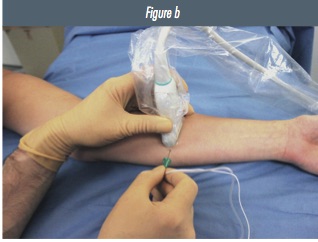
Figure 1: Patient, transducer and needle positioning for in-plane approach to median nerve of the right arm at a) the antecubital fossa and b) the mid-forearm.
Preliminary Scan
PRELIMINARY SCAN
Identify the brachial artery (pulsatile anechoic). The median nerve lies medial to the artery as a distinct hyperechoic structure. It is oval shaped, at a varying distance 0.5–2 cm from the artery. It is seen lateral and deep to pronator teres muscle. The ‘peak’ of the medial epicondyle of the humerus can be seen medially.
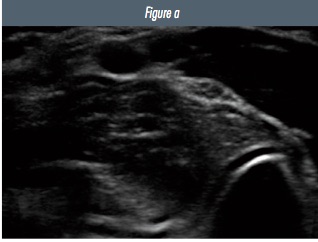
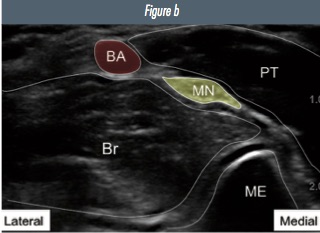
Figure 2: a) ultrasound image of the median nerve and surrounding structures in the antecubital fossa b) annotated image (BA=brachial artery; MN=median nerve; PT=pronator teres muscle; Br=brachialis muscle; ME=medial epicondyle of humerus).
Ultrasound Appearance
ULTRASOUND APPEARANCE
An ovoid, hyperechoic structure, with a speckled internal architecture. You will find it medial to the brachial artery. As you scan distally the median nerve travels deep and away from the artery. It can be traced into the middle of the forearm where it lies between the superficial and deep flexor muscles to the hand.
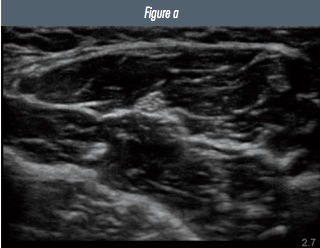
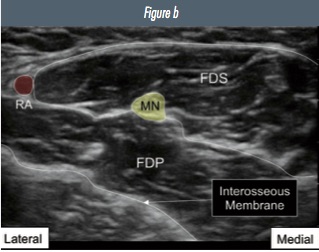
Figure 3: a) ultrasound image of the median nerve and surrounding structures in the mid- forearm b) annotated image (MN=median nerve; FDS= flexor digitorum super cialis; FDP= flexor digitorum profundus).

Text and images have been reproduced from the 2nd edition of the RA-UK Handbook, which can be purchased on Amazon, or is received on joining RA-UK. This excellent resource also contains practical descriptions of all of the advanced blocks referenced in the editorial.

 Introducing our brand new RAUK App. The free resource for all members to learn regional anaesthesia. Download the RAUK App on iOS or Android by clicking on the buttons..The App can be downloaded for free and non-members can view the Plan A content after registration. Members can unlock the full content by joining RA-UK where your RA-UK account will be linked.
Introducing our brand new RAUK App. The free resource for all members to learn regional anaesthesia. Download the RAUK App on iOS or Android by clicking on the buttons..The App can be downloaded for free and non-members can view the Plan A content after registration. Members can unlock the full content by joining RA-UK where your RA-UK account will be linked. 
{kind=link}