Superficial Cervical Plexus
Anatomy
ANATOMY
The superficial cervical plexus supplies sensation to the neck and shoulder. It is formed from the anterior rami of C2-C4 nerve roots. The branches of the plexus pierce the cervical fascia to emerge posterior to the mid-point of sternocleidomastoid muscle.
The sensory branches of the superficial cervical plexus are the lesser occipital, greater auricular, transverse cervical and supraclavicular nerves.
Positioning
POSITIONING
Patient supine, head turned to the contralateral side. Transducer initially applied at the level of the cricoid cartilage in the axial, oblique plane. Similar to the positioning for an interscalene block.
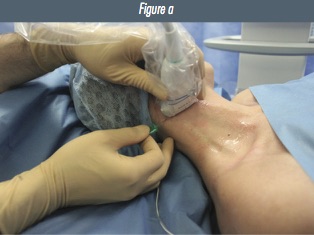
Figure 1: a) patient, transducer and needle positioning for in-plane superficial cervical plexus block.
Preliminary Scan
PRELIMINARY SCAN
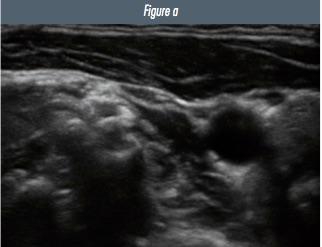
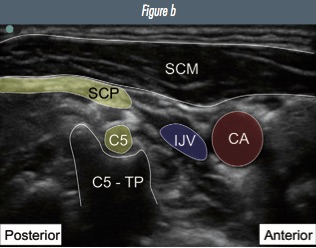
From the level of the cricoid cartilage, identify the interscalene groove and brachial plexus. Scan cranially and observe the C6 and then C5 nerve roots move deep towards their respective transverse processes (see interscalene chapter for images). At the level of the C5 transverse process, the superficial cervical plexus can be seen superficially as a line of hyperechoic beads in the fascial plane deep to the SCM muscle.
Figure 2: Ultrasound image of a) superficial cervical plexus b) annotated image (CA=carotid artery; IJV=internal jugular vein; C5-TP=C5 transverse process; C5=C5 nerve root; SCP=super cial cervical plexus; SCM=sternocleidomastoid muscle).

Text and images have been reproduced from the 2nd edition of the RA-UK Handbook, which can be purchased on Amazon, or is received on joining RA-UK. This excellent resource also contains practical descriptions of all of the advanced blocks referenced in the editorial.

 Introducing our brand new RAUK App. The free resource for all members to learn regional anaesthesia. Download the RAUK App on iOS or Android by clicking on the buttons..The App can be downloaded for free and non-members can view the Plan A content after registration. Members can unlock the full content by joining RA-UK where your RA-UK account will be linked.
Introducing our brand new RAUK App. The free resource for all members to learn regional anaesthesia. Download the RAUK App on iOS or Android by clicking on the buttons..The App can be downloaded for free and non-members can view the Plan A content after registration. Members can unlock the full content by joining RA-UK where your RA-UK account will be linked. 
{kind=link}